Horror at the Hotel Metropole: a medical murder mystery
Room 911 of Hong Kong's Hotel Metropole was the epicenter of SARS - 20 guests on one floor were infected in one night. Some died. Some carried it overseas to infect and kill others.


The majority of all SARS cases stem from a single mass infection event that took place on the night of 21st February 2003 at the Hotel Metropole in Kowloon, Hong Kong. The incident remains officially unexplained. Investigators never considered the possibility of terrorism.
Ground Zero
The story of Dr Liu Jianlun, who purportedly infected over 20 guests on a single floor of the hotel, aroused great interest in Hong Kong and was recounted in many media reports. However, journalists embellished their reports with unsourced facts and made assumptions to fill in gaps in the story.
On 21st February 2003, Liu - a retired doctor and professor - and his wife traveled by bus from Guangzhou to Hong Kong to attend a nephew’s wedding. On arrival they went shopping and had dinner with his sister and brother-in-law before checking into the Hotel Metropole for the night. A detail overlooked in most news reports is that of the 487 rooms in the hotel, he was given room 911. That number had become associated with terrorism to the extent that airlines stopped using it as a flight number. But if we assume SARS a natural disease outbreak the room number is a meaningless coincidence.
The next morning Liu stumbled into a nearby hospital, struggling for breath. During his overnight stay at the Metropole he had (reportedly) infected around 20 people, most of them international travelers, and all on the 9th floor. No other hotel guests, and none of the staff were infected. Some of those infected would travel on to seed new clusters in Hanoi, Singapore and Toronto, and elsewhere in Hong Kong. Over half of all SARS cases stem from this incident.
Hong Kong’s Legislative Council (LegCo) later held an inquiry into SARS to which the hospital staff who treated Liu provided statements, and some testified in person. At WHO’s instigation, Canada’s National Microbiology Lab (CNML) sent a team of investigators to Hong Kong, albeit some weeks after the incident, by which time some evidence (such as viral RNA) may have been cleaned or degraded. The CNML team was led by Dr Heinz Feldmann, now the head of virology at NIAID’s Rocky Mountain Laboratories. WHO epidemiologists did international contact tracing to supplement the efforts of Hong Kong’s Department of Health, and scientists from HKU and CUHK weighed in.
The evidence from these sources wasn’t available in full at the time of greatest media interest, and not before a premature consensus had formed that SARS was a natural phenomenon. The evidence was never weighed in totality with an open mind to the possibility of terrorism.
Patient Zero
According to the testimony of hospital staff, Liu arrived at the Kwong Wah Hospital (KWH) around 11 a.m. accompanied by two women the triage nurse thought were his wife and sister. His symptoms were heart palpitations, mild chest pain, and shortness of breath (dyspnea). He wasn’t coughing and sneezing, or nauseous and vomiting, as some have speculated when trying to explain his extreme infectiousness.
The triage nurse wrote recorded that he had started to feel ill 3 days earlier, but this conflicts with what he told doctors: that he had felt fine before leaving Guangzhou and spent the day shopping and dining with his family. The triage nurse noted an alarmingly low blood oxygen level, signaling that he should be admitted to the emergency ward immediately.
Once given an oxygen mask his oxygen levels recovered. Liu told doctors he was a retired professor of nephrology (kidneys). He had been helping out in an outpatient clinic at the teaching hospital - Guangzhou’s Sun Yat-Sen University Second Affiliated Hospital (SYSU2). There he had treated two patients with atypical pneumonia (atypical implies a dry unproductive cough, rather than a large amount of phlegm) of unknown cause. He claimed he had also had a bout of pneumonia about a week earlier, but had fully recovered before traveling. He was adamant he didn’t have the atypical pneumonia that had recently made the news.
Fortunately for KWH, some of their doctors had seen reports in Hong Kong media 10 days earlier.

Liu was moved swiftly to a negative pressure isolation room. Staff were warned to take extra precautions. There were several serious nosocomial outbreaks of SARS. KWH escaped lightly.
Liu continued to insist that he didn’t have the mysterious “atypical pneumonia” - until confronted with an X-ray.
An epidemiological report on the outbreak at Liu’s workplace SYSU2 claims that 90 staff, and 6 others had been infected there, although there was just one death. It was well known in Guangzhou that healthcare workers had been disproportionately affected, millions of text messages had been sent to tell people to avoid hospitals. Would Liu have risked attending a family wedding banquet, having treated atypical pneumonia patients and himself having had pneumonia just days earlier?
Some LegCo councilors suggested that Liu may have not come to Hong Kong for a wedding, but seeking treatment for the mystery disease that had left Guangzhou doctors baffled. Some even suggested KWH may have been forewarned of his arrival. The doctors rejected this.

Coincidentally (perhaps) KWH had a “sister hospital” arrangement with Sun Yat-Sen University First Affiliated Hospital (SYSU1). Monday morning following his admission, KWH’s head of surgery, received a call from SYSU1 enquiring after Liu.
The caller asked that KWH call in microbiologists from Queen Mary Hospital (affiliated with HKU) to see if they could diagnose Liu’s disease. Dr Ye contacted old friend, K.Y. Yuen, who sent two microbiologists to examine Liu and take samples.
Then at 6 p.m. three senior doctors from SYSU1 arrived from Guangzhou on what they claimed to be a social visit to pay their respects to an old colleague. Liu was by that stage intubated and semi-comatose, unable to speak.
The Guangzhou doctors were most interested in any diagnosis,and asked for a copy of his test reports. It was inconclusive but ruled out avian influenza and other common causes of pneumonia.

When asked about the situation in Guangzhou hospitals, the visitors didn’t offer any information, other than to say that some were claiming the mystery disease was caused by Chlamydia, but they didn’t share this view.
On the trail of the Poison King
How did Dr Liu Jiunlun himself come to be infected in Guangzhou? It’s a bizarre saga - if the official account is to be believed.
The index patient in the Guangzhou outbreak was said to be a fishmonger named Zhou Zuofen - who came to be known as the “Poison King”. His age is stated in different sources as 42, 44 or 46. He was admitted to SYSU2 on January 30th, staying less than 36 hours. In that time, he managed to infect 35 people directly - every member of staff who had even brief contact with him. The epidemiology report by the hospital counted 90 staff but only 6 of their family members infected in total - a surprisingly short chain of transmission from a large number of primary infections.
There was only one death recorded, the unfortunate 55 year-old ambulance driver who, on the morning of February 1st, transported Zhou Zuofen across Guangzhou from SYSU2 to SYSU3. Why was Zhou transferred to another hospital? According to the SYSU2 reports, it was because SYSU3 had been specially designated to treat atypical pneumonia patients. But that isn’t supported by other sources. The 90 infected staff at SYSU2, including the ambulance driver, were treated at their own hospital - not transferred. There were other hospitals that were closer, and better equipped. The 8th People’s Hospital was an infectious disease hospital with capacious negative-pressure isolation wards. Some SARS patients were transferred to Zhong Nanshan’s Guangzhou Institute of Respiratory Disease, less than 1km from SYSU2.

A media ban on reporting on SARS was in place for most of the epidemic. It was only after it was lifted around April 20th that the story of the “Poison King” became known. He had (it was claimed) single-handedly spread the infection to 3 Guangzhou hospitals and beyond.
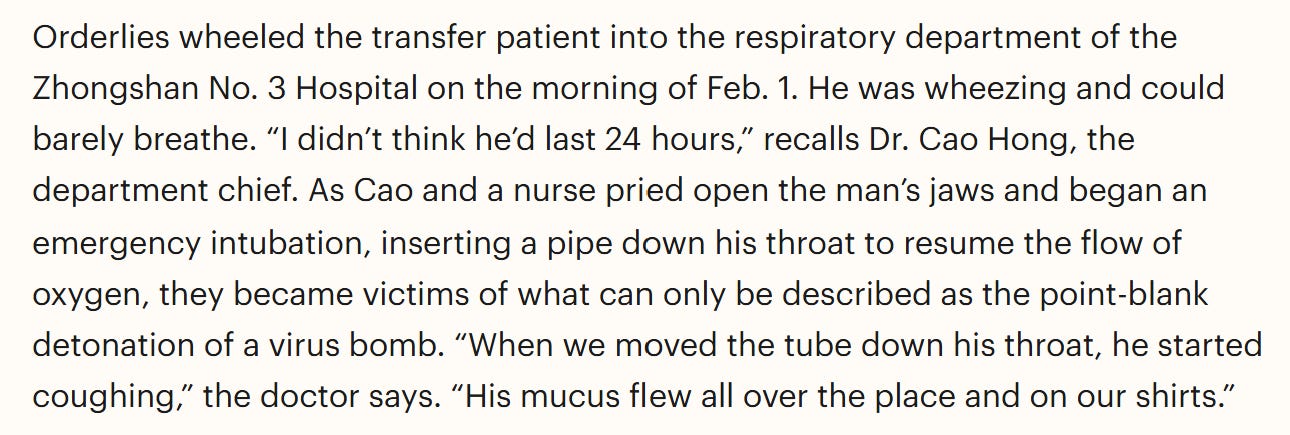
There was an anecdote about staff at SYSU3 struggling to intubate him resulting in many infections. But versions of the story differ in important details. In one account in Time Magazine, published on April 21st, the respiratory department head named Cao Hung performed the unpleasant procedure.
This conflicts with an even more graphic account from Guangzhou’s Southern Daily on April 24th. Cao Hung isn’t mentioned. It celebrates the heroic efforts of Deng Lianxian - the Deputy Director of the Infectious Disease Department - and also the CCP branch secretary.
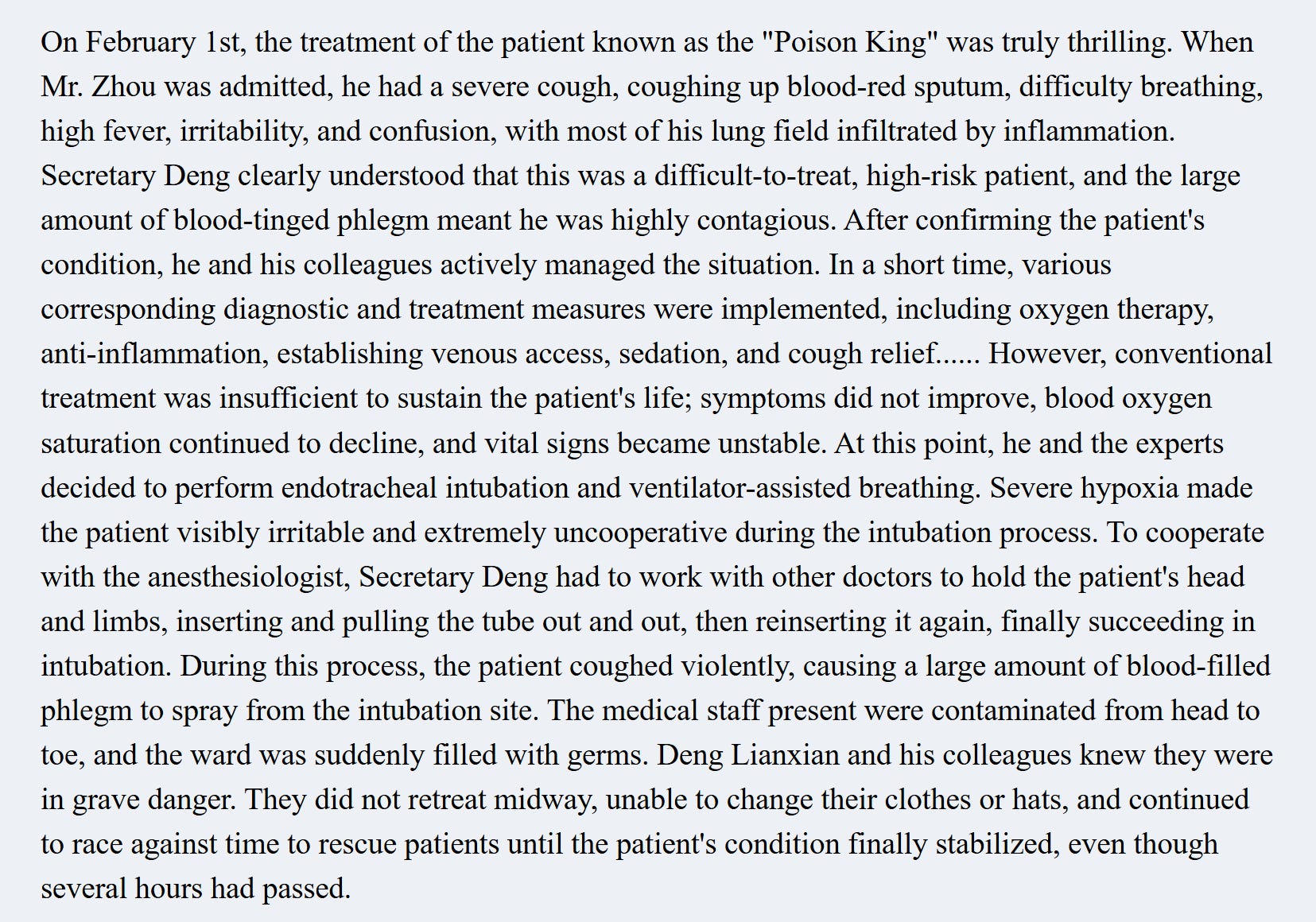
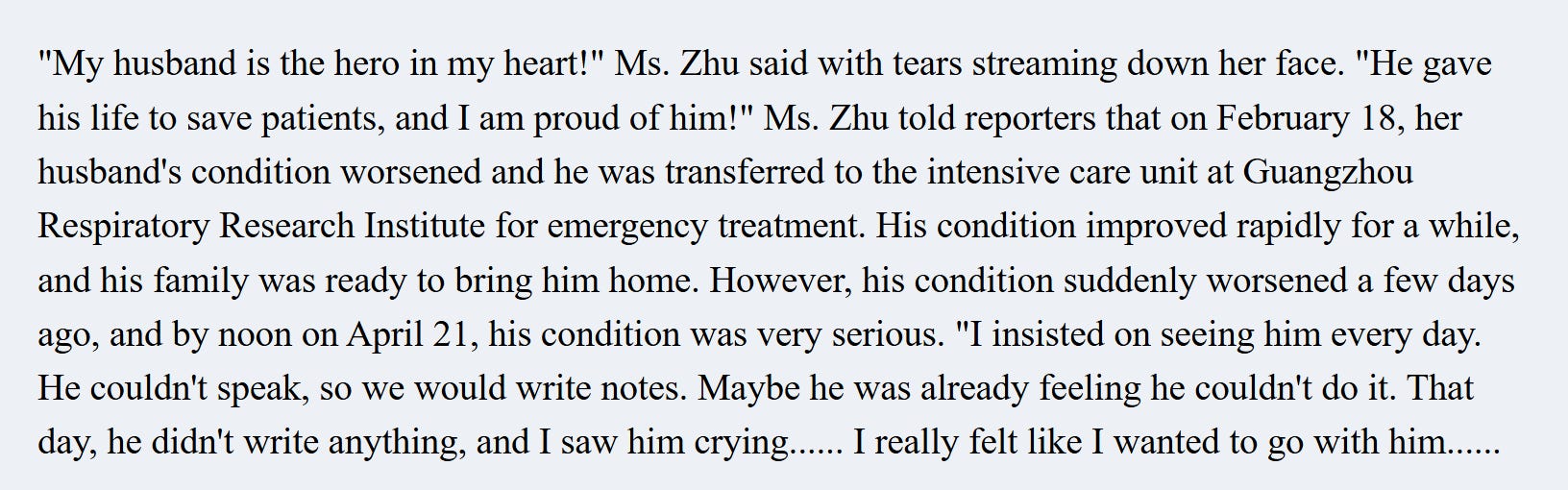
This article is the heroic Deng Lianxin’s obituary. According to this Deng died of SARS on April 21st. That is almost 3 months after he became infected. He had been transferred to Guangzhou Respiratory Research Institute, at first staging a complete recovery before having a sudden relapse from which he never recovered. The course of Deng’s extended illness is similar to that of certain Wuhan doctors who died in the early phase of Covid-19.
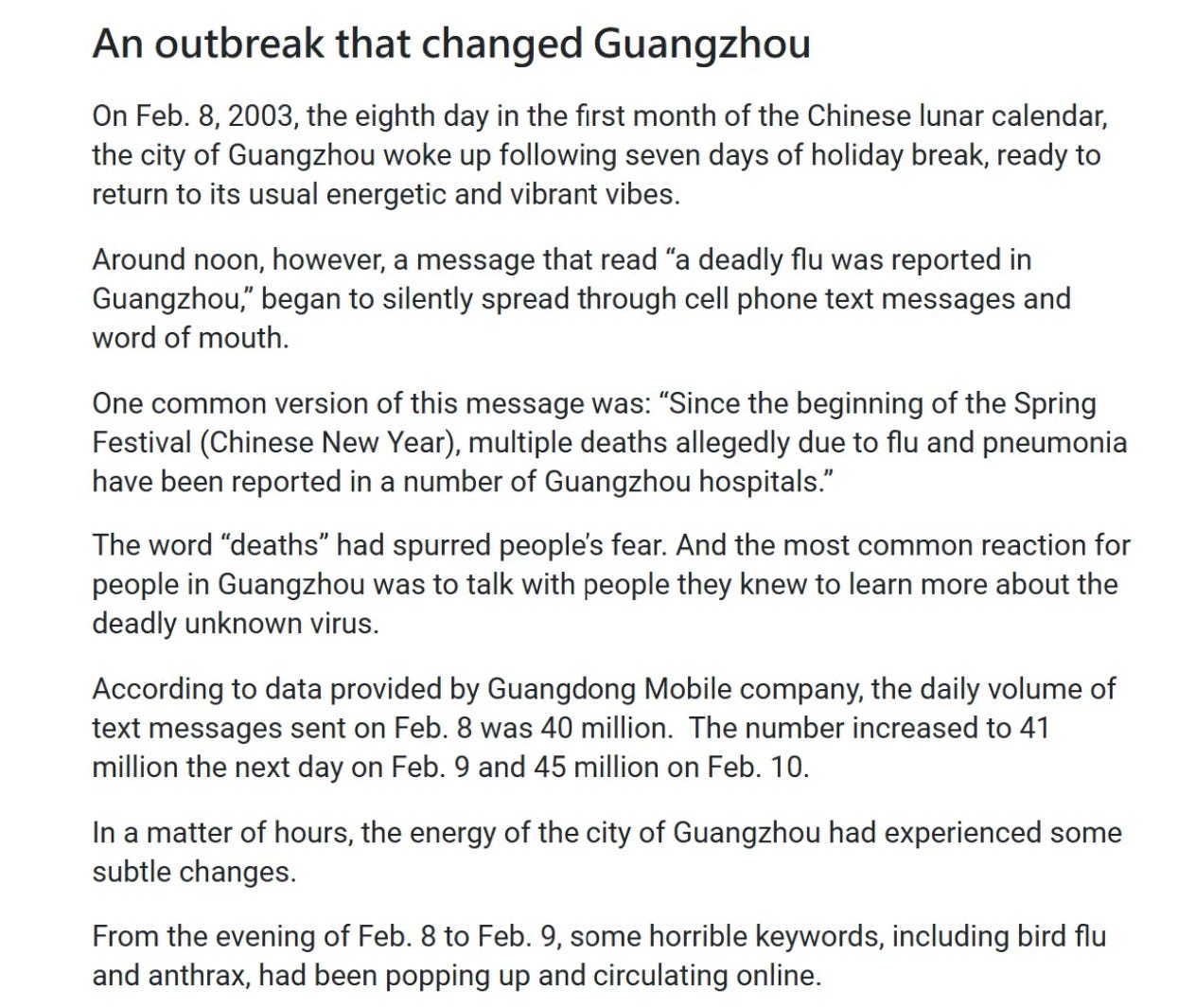
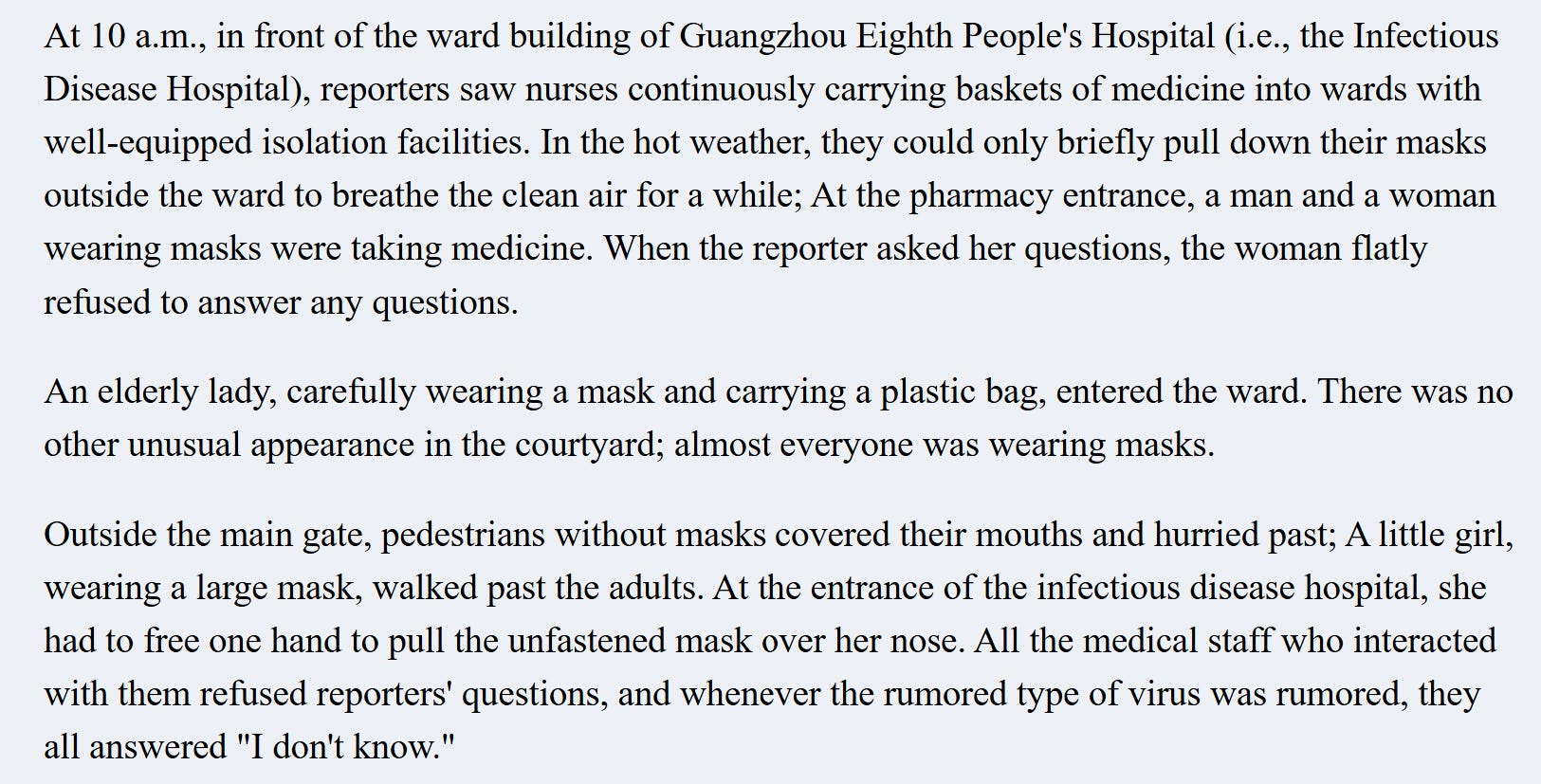
On February 8th the Poison King was transferred to a third hospital - the 8th People’s Hospital. That day, Southern Daily reported that what appears to have been an organized text message campaign, warning people about a deadly pneumonia afflicting Guangzhou hospitals.
During the brief window they were allowed to report on the illness, Southern Daily sent a reporter to the 8th People’s Hospital. It seemed busy. A WHO report stated that during the second week of February, 150 of 400 beds in isolation wads were occupied by SARS patients.
They also visited SYSU3 but found quite different conditions.

They didn’t visit SYSU2, and there is mention of an outbreak there.
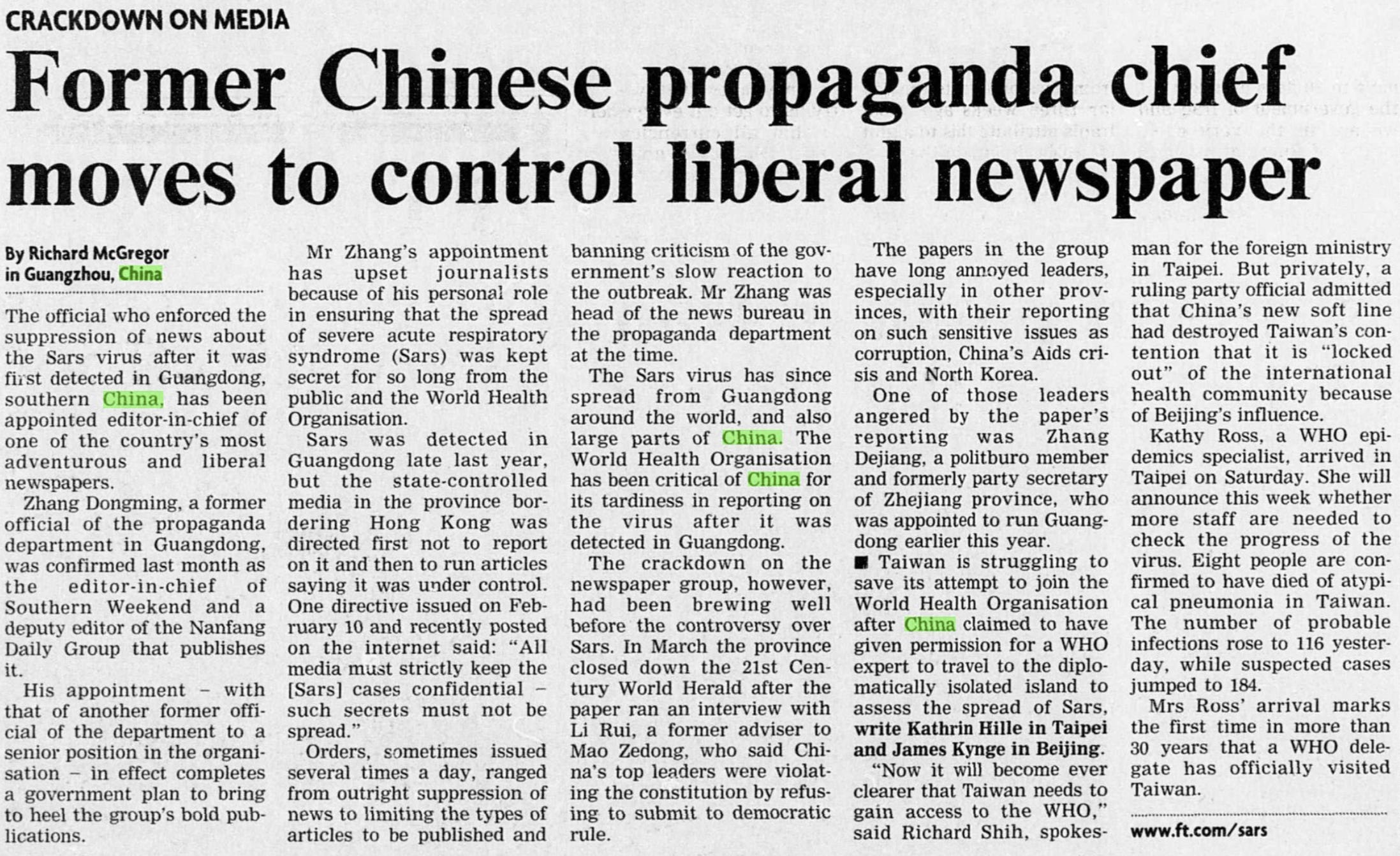
Following publication of this article, authorities re-imposed a strict ban on reporting on the disease. It wasn’t until April 20th that the new President Hu Jintao ordered the media blackout relaxed. But the censorship didn’t end, propaganda department officials were installed at the Southern group in senior editorial positions.
Chinese and Hong Kong journalists tried to interview the Poison King, as did the WHO. But he evaded them all. It was only in 2013, in a 10th anniversary retrospective, that more color was added to his story.
The 8th People’s Hospital is very close to Guangzhou’s World Trade Center complex (which is owned by a state-owned enterprise) the subject of rumors of a mass infection event - with some even suggesting bioterrorism.

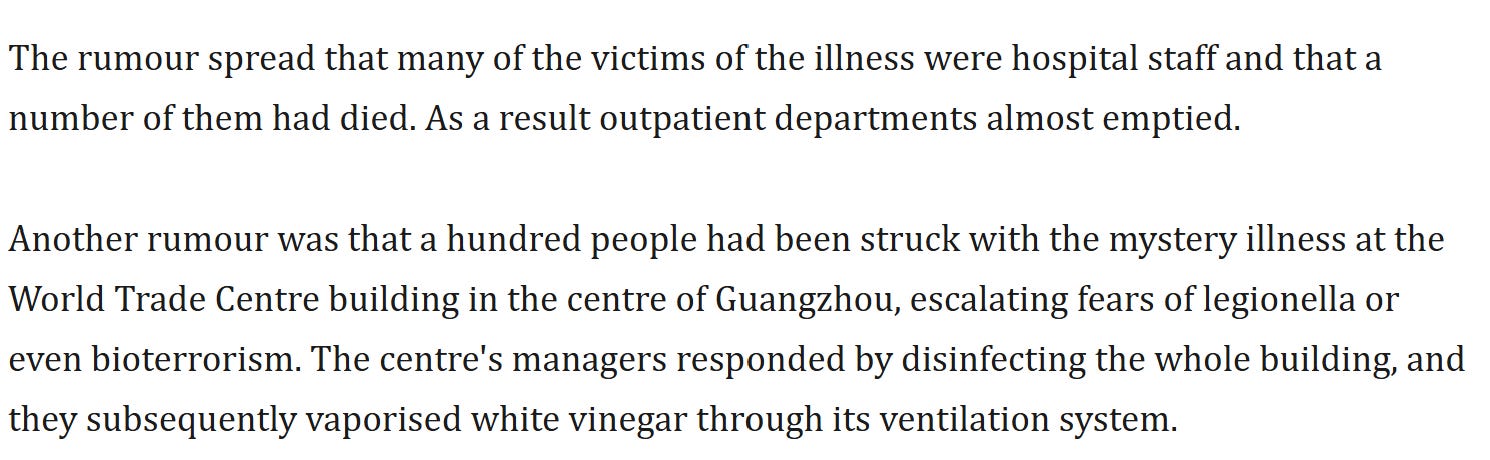
Although there is scant evidence either way, the spatial and temporal pattern of infections is consistent with these rumors and inconsistent with a regular respiratory outbreak spreading across the city. The total number of infections in Guangdong is trivial for a province its size (~80 million). Alarms were only triggered because cases were concentrated at a handful of hospitals during a brief window - and that they were advertised in a mass text messaging campaign. For most people life returned to normal as soon as the government responded by announcing the numbers - just 305 cases and 5 fatalities (as 12th Feb, 2003).
The Weakest Link
Aside from the inconsistent and conflicting details in the story of the Poison King, there are other complications in trying to link him to Dr Liu Jianlun and the Hotel Metropole.
Zhou left SYSU2 on February 1st. Liu didn’t report symptoms of pneumonia until February 15th. The time to symptoms onset is generally 2-5 days from infection. Liu had no contact with Zhou, but he must have known SYSU2 suffered a major outbreak. Why didn’t he communicate this to KWH doctors?
According to the SYSU2 reports all 90 staff and 6 family members infected were hospitalized for an average of 17 days in isolation wards spread over 4 floors of the hospital. This suggests the hospital took quarantine very seriously. How did Liu avoid the same?
The CFR recorded at SYSU2 was just 1% (1 death from 96 cases). In contrast, not only did Liu die, so did 3 others infected by him, and there are 13 more deaths from tertiary transmissions.
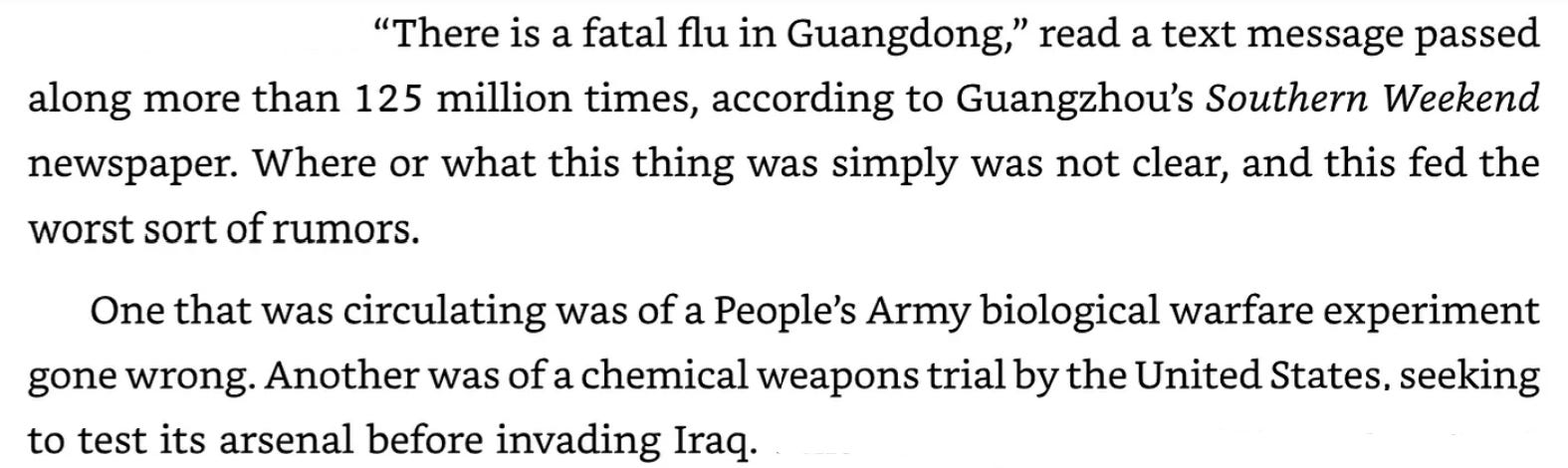
Although Liu’s samples were never sequenced, cases descended from him have several mutations compared to those sequenced from patients at SYSU2. An AMMS/Institut Pasteur paper attempts to explain these as human adaptations following a recent zoonotic spillover, and claims that the same mutations evolved independently (convergently) during an epidemiologically separate Beijing outbreak. However as most of these mutations are synonymous, this seems unlikely.
Downstream Clusters
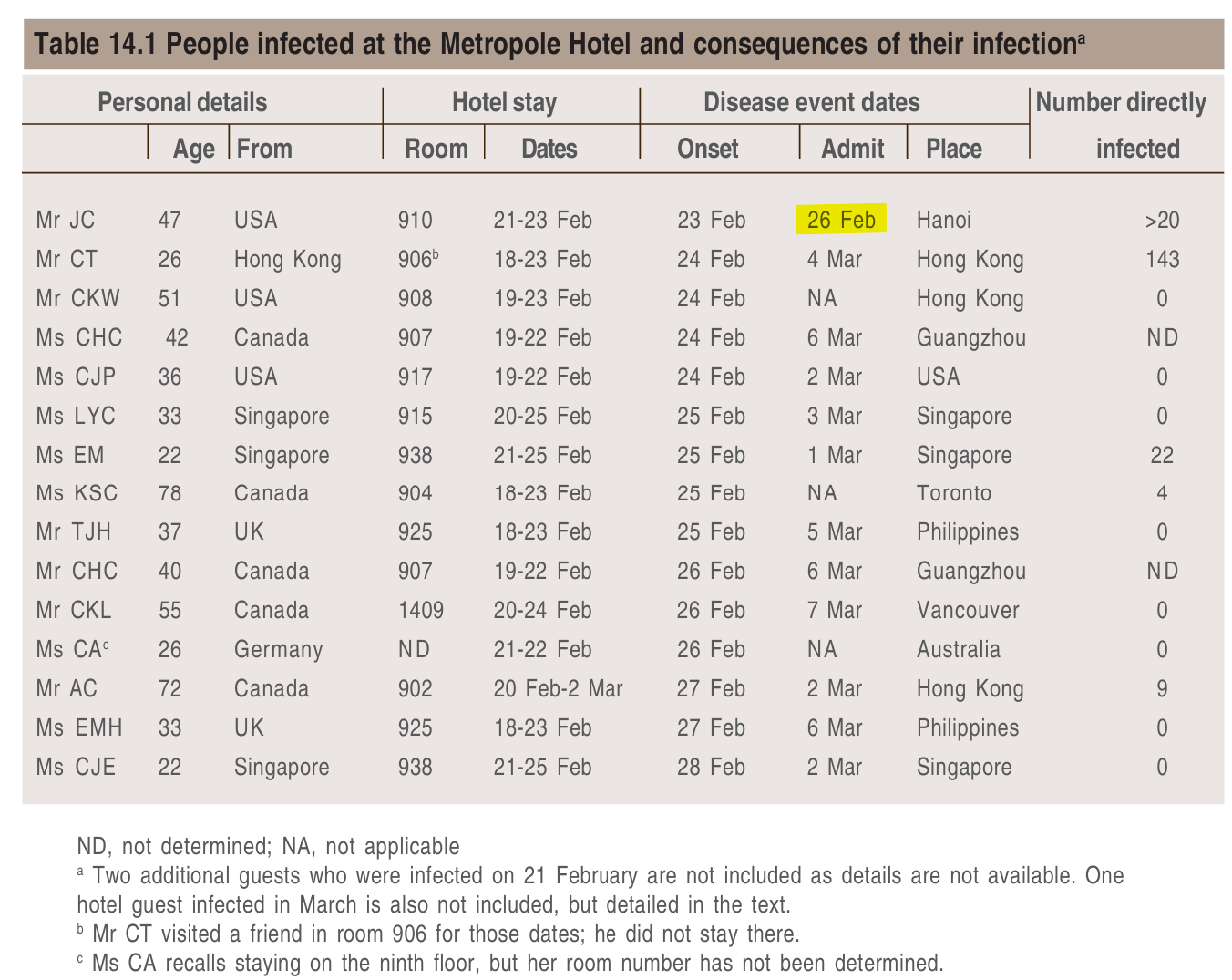
Another extraordinary aspect of Liu’s case is that of the ~20 people he infected at the Hotel Metropole, five went on to become super-spreaders in hospitals in four different cities: Toronto, Hanoi, Singapore, and Hong Kong, but the other ~15 victims transmitted to no-one else.
Tragically, infections were fatal for some super-spreaders and/or their immediate family/carers.
23-year-old Esther Mok returned to Singapore. She survived, but infected her mother, father, uncle and pastor who all died. She also seeded a major cluster in Singapore’s Tan Tok Sen Hospital, infecting 24 healthcare workers directly, but with no fatalities.
48-year-old Johnny Chen traveled on to Hanoi, became ill and wound up in the French Hospital. He died, as did two nurses aged 43 and 46, and four doctors aged 36, 46, 66, 69. All those who died were directly involved in his treatment and care. In total 63 people were infected in the cluster - staff, patients and their family members. Only 6 of these were infected outside the hospital.
87-year-old Kwan Sui-Chu flew to Toronto. She died at home, as did her husband. Her son, aged 43, triggered a major outbreak at Toronto’s Scarborough Grace Hospital, and later died too. Of 128 cases in the cluster, only 41 hadn’t visited the hospital, but were close family of staff or patients.
26-year-old Chow Yin-au visited a friend who was a guest but didn’t stay overnight at the hotel himself. He was admitted to Hong Kong’s Prince of Wales hospital on March 4th. There he directly infected 112 people of a total of 148 in the cluster. There was only one fatality, a ward worker, aged 55.
How can we account for these unusual features of epidemiology?
A high fatality rate among immediate family members, and in one instance direct carers of super-spreaders.
Few tertiary cases (aside from some super-spreader incidents further downstream, which may also be acts of terrorism).
Community spread among those who haven’t visited affected hospitals is extremely rare.
Low fatality rate among cases not infected by a super-spreader (aside from some elderly patients who were already hospitalized for a pre-existing condition).
Transmission at the Metropole
The super-spreaders from the Metropole have little in common in term of age and sex - the index case is Male, 64 and the secondary super-spreaders are F23, M43, M26, F87, M72.
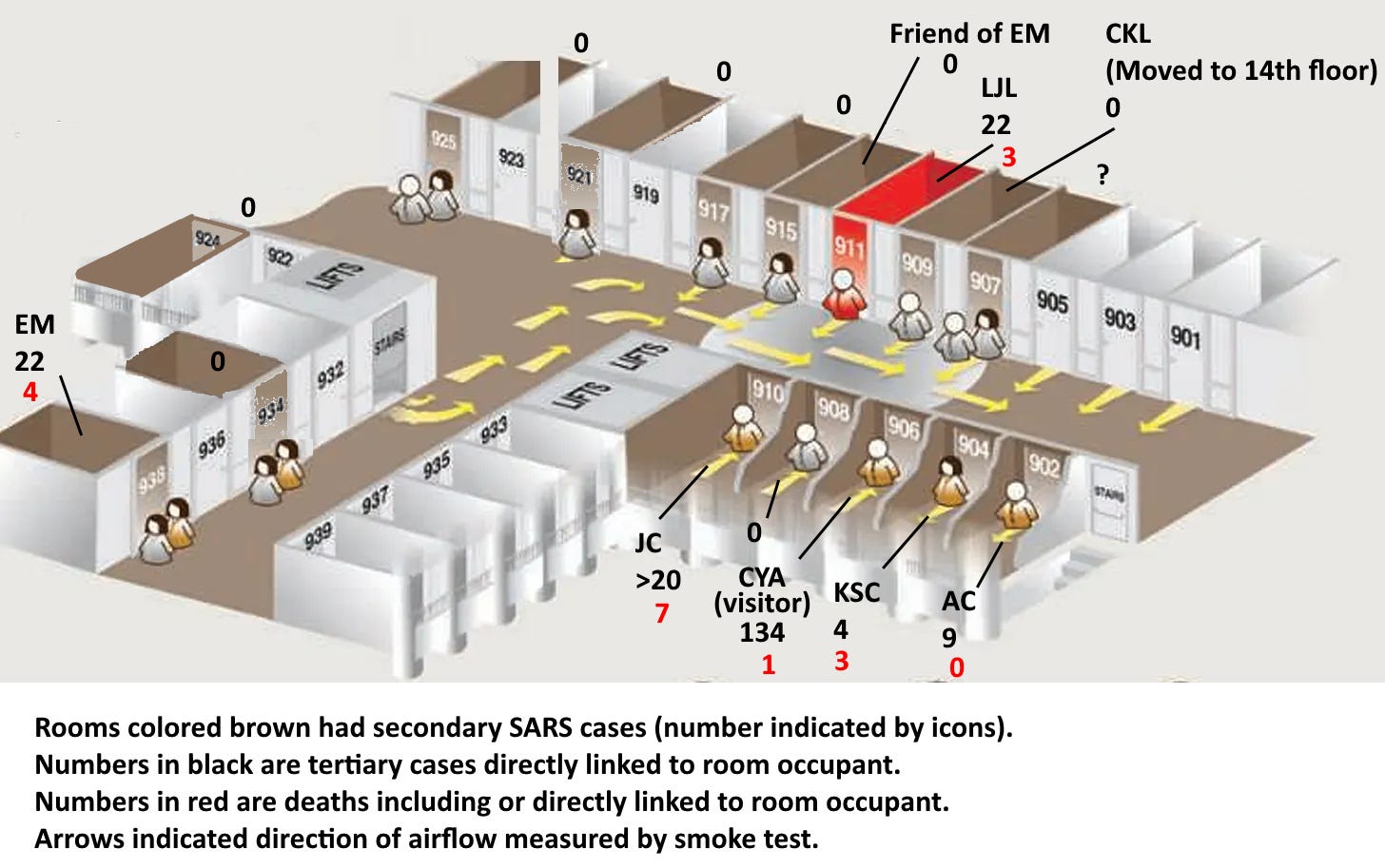
The hotel floorplan shows 4 of the 5 secondary super-spreaders are on one side of the hallway “downwind” of Room 911. The other secondary super-spreader, Esther Mok (EM) was not near these rooms, but her friend stayed in 915, next door to 911 it’s possible she visited or left some luggage there. Note there’s no room 913 (numerology matters!).
It seems a reasonable (though unproven) hypothesis that severity is correlated with initial dose - but at the Metropole there was no close contact reported between Liu and the others, and transmission was almost certainly by aerosol. Moreover, the guest rooms were shown to be at higher pressure, air flowed outwards from them. Could Liu really have been exhaling virus at such levels as to infect people through his closed door as they passed through the hallway? Why didn’t he infect staff and others he had contact with on his journey?
Most infected guests were from the US, Canada, Singapore, UK - these are countries that might be targets for terrorists in the lead-up to the Iraq war (Singapore was a strong supporter of the invasion). All but one of those infected left the hotel within 4 days of the incident, ensuring they reached their destinations before the onset of symptoms. Some traveled on, rather than returning immediately to their home country which is why the US avoided the deadliest cluster.
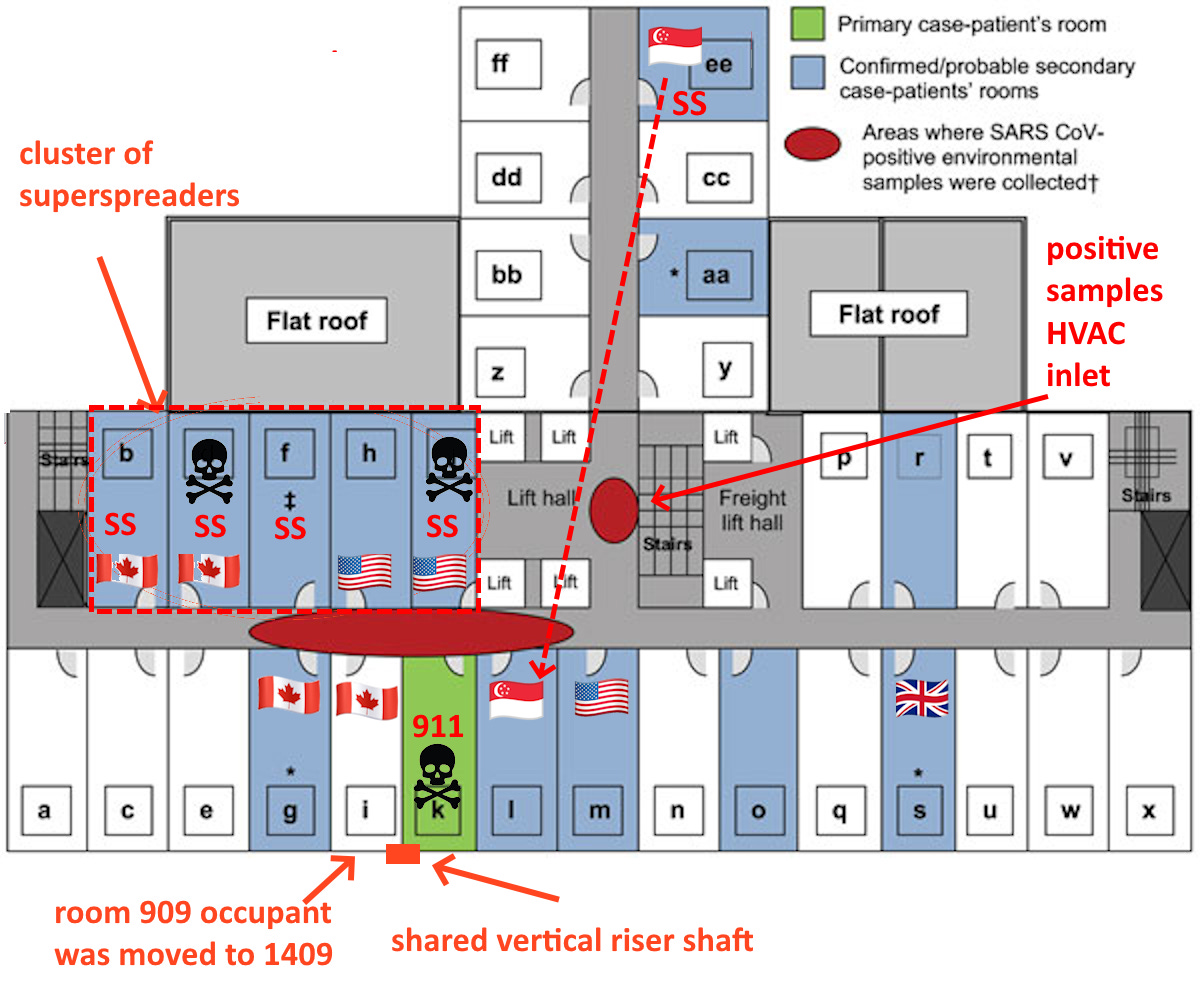
One possibility is that aerosolized virus was introduced via the HVAC system. Rooms nearest to the inlet received the highest concentration of virus. The deadliest downstream super-spreader Johnny Chen, stayed in the room directly opposite room 911, but also closest to the HVAC air exchanger. He was hospitalized sooner than the others, aside from Liu himself. A positive sample of viral RNA was taken on the HVAC inlet filter. No viral RNA was detected in any of the rooms, but it’s possible it had degraded after repeated cleaning, as the rooms were in use for some weeks afterwards. The investigation team seemed somewhat surprised that any RNA had been detectable.
The Hotel Metropole was (and is) owned by Chinese state-owned enterprise China Tourism Group, as such, it’s possible some of the hotel staff were accomplices in the plot. Interestingly during the night, a guest in a room neighboring Liu was transferred to the same room number on the 14th floor. The guest, a Canadian, didn’t recall this.

The CNML investigators observed that room 909 and 911 shared a vertical riser shaft. This might allow a terrorist to release an aerosol from room 909 into room 911, or potentially from a room sharing this shaft above or below.
Report by CNML investigation team.
Why did some people infected go on to become super-spreaders themselves, and why were they often deadly to those they transmitted to?
I speculate that other than the virus replicating within their bodies, there was some exogenous source of aerosolized virus they took with them from the Hotel Metropole.
It may be simply that aerosolized particles from the initial attack permeated their hair, clothes and luggage, dispersed and decayed over a period of days to weeks. The time from contamination at the Metropole to close contact with family members or direct carers correlates with severity and fatality. This likely correlates with the initial dose they received. Soviet bioweaponeers discovered that as few as 5 particles of virus were enough to produce severe monkey pox infections in monkeys, but with a less well adapted pathogen (such as SARS is in humans) small doses may be efficiently deal with by the immune system, causing little more than a mild fever.
This scenario requires that the source of the infection is a dry aerosol bioweapon. The virus is freeze-dried, encapsulated in a protective medium in particles that are an optimal size for dispersal, inhalation and deposition deep in the lungs. Dry aerosols are prized by bioweaponeers for long-term stability, they can be stored indefinitely at room temperature. It isn’t straightforward to engineer, particularly when the agent is an enveloped virus (which are easily destroyed by shear forces during milling, or when exposed to organic solvents).
But there are ways - some of which were developed in the course of research into vaccines using viral vectors. Vaccines can be designed to be administered by inhalation. Microparticles encapsulating the virus are sized to be inhaled deep into the lungs, to adhere to the alveolar surface rather than being exhaled. Using synthetic polymers they can be designed to decompose gradually releasing a constant dose, a dose which increases over time, or even delivers a booster two weeks after the first dose. Natural polymers are also used, they are less controllable, but easier to manufacture.
Another possibility is that something was left in hotel rooms, adulterated with virus in solid or liquid suspension, that could be aerosolized at the travelers’ destination. Perhaps complementary toiletries, a spray or powder, or a gadget that they took with them and used on arrival at their destination and/or took with them to a hospital.
A future article will look at AMMS capabilities at all stages of the pipeline of engineering an aerosol bioweapon: sampling bats, culturing and adapting a virus, engineering the spike, and weaponizing as an aerosol. There is much evidence pointing specifically to AMMS. Given that, I continue to be mystified as to why the US was at most uninterested in the possibility of an artificial origin, if not actively colluding in the cover-up. An email to Anthony Fauci recently released by Senator Rand Paul claimed that only a cursory unclassified report was made by the IC, there was no classified version. Can they really have had no suspicions? Or are these secrets held in the 9th basement floor at Langley?

While there is no mention of terrorism in the unclassified report, a sidebar briefly discusses the difficulty distinguishing between natural disease emergence and the release of a bioweapon. In order to distinguish you have to consider both possibilities.